
Psychoneuroimmunology: The Science of How the Mind, Brain, Hormones, and Immune System Communicate.
For a long time, medicine tended to treat the mind and body as if they were separate worlds. Thoughts belonged to psychology. Hormones belonged to endocrinology. Immunity belonged to immunology. The brain was the brain, and the immune system was the immune system. Psychoneuroimmunology, usually shortened to PNI, helped change that picture. It emerged as a serious scientific field by showing that behavior, the nervous system, the endocrine system, and the immune system are in constant communication. In other words, the body is not a collection of isolated parts. It is a living network.
At its core, psychoneuroimmunology studies the interactions among psychological processes, the central and autonomic nervous systems, the endocrine system, and the immune system. It asks questions that are both simple and profound: How does chronic stress affect immunity? Why can loneliness or depression alter inflammation? Why does infection change mood, motivation, sleep, and behavior? And can psychological or behavioral interventions improve aspects of immune function? PNI does not rest on vague mind-body slogans. It is built on measurable pathways, molecules, nerves, hormones, immune cells, and observable changes in health and disease.
The field is often traced back to landmark work by Robert Ader and Nicholas Cohen in the 1970s. In their classic experiments, they showed that immune responses could be altered through conditioning. That finding mattered because it challenged the old belief that the immune system functioned independently of the brain. Their work helped establish the idea that the nervous system could influence immune activity, and it opened the door to decades of research on stress, emotion, behavior, immunity, and disease.
So how does this communication actually work?
One direction is top-down, from brain to immune system. When the brain perceives a threat, whether physical or psychological, it activates stress-response pathways. Two of the most important are the hypothalamic-pituitary-adrenal axis, or HPA axis, and the autonomic nervous system, especially the sympathetic branch. The HPA axis ultimately leads to the release of cortisol, while the sympathetic nervous system releases catecholamines such as norepinephrine. Immune cells carry receptors for these messengers, which means stress chemistry can directly alter immune activity. Sympathetic and parasympathetic nerve fibers also communicate with lymphoid tissues, giving the brain another route for influencing immune function.
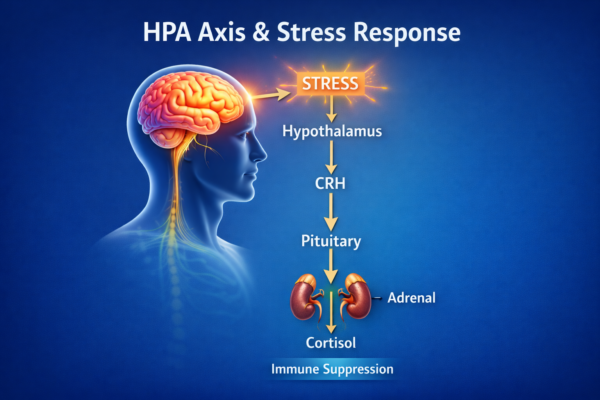
In the short term, this system is adaptive. If you face an acute challenge, your body reallocates energy, heightens vigilance, and prepares for injury or infection. But when stress becomes chronic, the picture changes. Repeated activation of the HPA axis and sympathetic nervous system can dysregulate immune signaling. Instead of a brief and efficient response, the body may drift toward immune suppression in some contexts, exaggerated inflammation in others, or both at different times and tissues. This is one reason chronic stress has been linked with greater vulnerability to illness, slower recovery, and a more inflammatory internal environment.
One of the most famous examples comes from viral challenge studies by Sheldon Cohen and colleagues. In those experiments, people experiencing higher levels of psychological stress were more likely to develop clinically verified respiratory illness after exposure to common cold viruses. Other work showed that chronic stressors were particularly important in increasing susceptibility. These studies became influential because they did not simply ask people whether they “felt unwell.” They used controlled viral exposure and objective outcomes, helping show that stress can have real biological consequences for host resistance.
Stress can also affect healing itself. In a classic study by Janice Kiecolt-Glaser and colleagues, psychological stress slowed wound healing. That finding added a practical dimension to PNI: stress is not only something a person feels internally. It can shape how efficiently the body repairs tissue. Over the years, Kiecolt-Glaser’s work and related research have helped show how chronic burden, including caregiver stress, can alter immune regulation, inflammation, and health outcomes over time.
The second direction is bottom-up, from immune system to brain. This is one of the most fascinating parts of PNI. When immune cells detect infection or injury, they release signaling proteins called cytokines, including molecules such as interleukin-1, interleukin-6, and tumor necrosis factor-alpha. These cytokines do not stay confined to the immune system. They communicate with the brain through several pathways, including afferent nerves such as the vagus nerve, transport and signaling at the blood-brain barrier, and signaling in brain regions that are more exposed to circulating immune information.
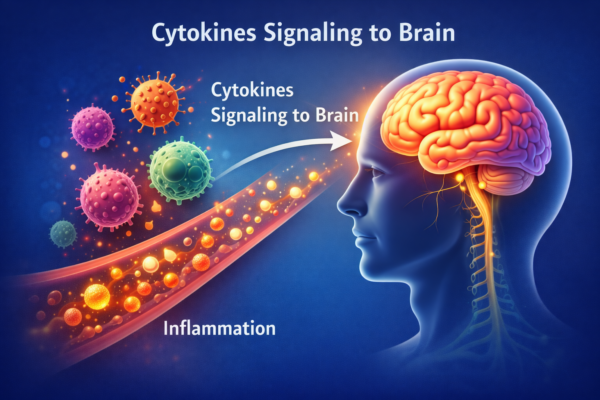
When the brain receives these immune signals, it shifts behavior in ways that are often protective in the short term. This is the biology of sickness behavior. Fatigue, reduced appetite, withdrawal from social activity, poorer concentration, sleep changes, low motivation, and a desire to rest are not random weaknesses. They are part of a coordinated response designed to conserve energy and support recovery. Researchers such as Robert Dantzer and colleagues helped establish that these behavioral changes are driven in part by inflammatory cytokine signaling to the brain. In prolonged inflammatory states, however, the same pathways may contribute to more persistent depressive symptoms and reduced quality of life.
This is one reason PNI has become so important in understanding depression and related conditions. Modern research suggests that, in at least some individuals, depression is not purely a neurotransmitter story. Inflammation can interact with mood, reward processing, motivation, sleep, and behavior. Stress can increase inflammatory activity, and inflammatory signals can, in turn, influence the brain in ways that resemble depression. This does not mean every case of depression is “caused by inflammation,” but it does mean the relationship is more biologically intertwined than older models allowed.
Another important PNI theme is social connection. Human beings are profoundly social organisms, and social experience has biological consequences. Reviews in this field suggest that adverse social experiences, including loneliness, social isolation, and perceived social threat, are associated with a pattern of increased inflammatory signaling alongside reduced antiviral responses. By contrast, supportive social connection may help reduce inflammatory burden and strengthen antiviral defense. In plain language, the body appears to register disconnection as a kind of biological stressor.
This matters because many people assume “stress” means only feeling mentally overwhelmed. PNI shows that stress is broader than that. It includes perceived threat, uncontrollability, unresolved burden, relational pain, and the wear-and-tear of living in a prolonged state of vigilance. It also helps explain why two people can face the same external circumstances yet show different biological outcomes. The immune system is not responding only to pathogens. It is also responding to the wider context in which a person is living, coping, sleeping, relating, and interpreting experience.
Naturally, this leads to another question: if psychological states can influence immune pathways, can psychological or behavioral interventions help?
The answer is yes, to a degree, but the science needs to be described carefully. A major 2020 systematic review and meta-analysis in JAMA Psychiatry, covering 56 randomized clinical trials and 4,060 participants, found that psychosocial interventions were associated with beneficial changes in immune function over time. These changes included decreases in harmful inflammatory activity and improvements in beneficial immune outcomes. The most consistent effects were seen with cognitive behavioral therapy and with combined or multi-component interventions. That is an important finding, but it still does not justify exaggerated claims. The average effect was meaningful, not magical.
Mindfulness-based interventions have also drawn substantial interest. A systematic review of randomized trials concluded that mindfulness meditation showed possible effects on markers of inflammation, cell-mediated immunity, and biological aging, but the evidence was heterogeneous and the authors emphasized that results were still tentative and needed replication. That is the right way to talk about this area: promising, plausible, and in some cases measurable, but not settled in every detail.

There are also individual studies that suggest more specific immune effects. In a well-known randomized trial, Richard Davidson and colleagues found that an 8-week mindfulness program was associated with changes in brain activity and greater antibody response to influenza vaccination compared with a wait-list control group. Studies like this are part of the reason interest in contemplative practices grew inside PNI. Still, single studies should be interpreted in the context of the broader literature, which is why systematic reviews remain essential.
All of this brings us to an important caution. PNI does not mean that thoughts alone cure disease. It does not mean a person is to blame for becoming ill. It does not mean that stress management replaces evidence-based medical care. What it does mean is that biology is responsive to lived experience. It means the brain, endocrine system, and immune system are woven together. It means that psychological distress can alter physiology, and that reducing distress may support better regulation of inflammation, immunity, and recovery. In serious illness, including conditions marked by ongoing inflammation or immune activation, these interactions may matter substantially for symptoms, resilience, healing capacity, and quality of life.
This is why psychoneuroimmunology is so clinically and personally significant. It gives scientific language to something many people have sensed intuitively: the body listens. It listens to threat. It listens to safety. It listens to isolation and to connection. It listens to persistent fear, but it also responds to regulation, support, meaning, and care. The message of PNI is not mystical. It is biological. The mind and body are not separate conversations. They are different expressions of the same one.
In that sense, PNI offers both realism and hope. The realism is that chronic stress, depression, loneliness, and unresolved burden can leave measurable fingerprints on the immune system. The hope is that intervention matters. Psychological support, improved coping, stress reduction, social connection, and evidence-based mind-body practices may influence the biology of health in ways that are now increasingly measurable. Not perfectly. Not universally. But enough to make the field impossible to ignore.




{kind=link}